CVC in Public Hospitals

Photo Credit: Image by Freepik
On this page: A look at a hypothetical integration of public and private hospital in the public hospital area in a developing country to demonstrate practical challenges and concrete opportunities of CVC. Read more below, or visit the Guidelines on Innovative Revenues for Infrastructure section and the Content Outline, or Download the Full Report.
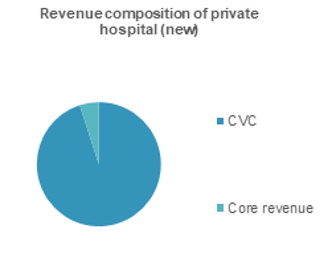
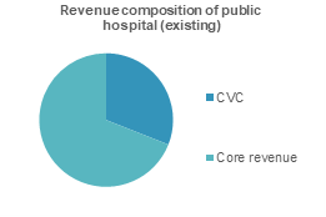
Developing countries face a wide range of complex healthcare challenges spurred by changing demographics, a growing burden of chronic disease, rising healthcare costs, more informed patients, and rapidly changing healthcare technologies. Healthcare systems are increasingly strained and struggling with how to expand access and deliver high-quality healthcare services – all while controlling costs. Additional investment in health will be needed in developing countries where healthcare infrastructure remains inadequate, and facilities lack access to the necessary management skills and patient care workforce to address the growing demands of caring for their population. Governments are looking for ways to mobilize and encourage private investment in delivery of public health services. This Worked Example looks at a hypothetical case in a developing country which involves the integration of a public and private hospital in the public hospital area. Project Scope: The project will expand additional beds in the same area as the existing public hospital, to a similar capacity as the existing hospital. The new hospital will be developed as a co-located and co-branded hospital through a joint venture (JV) between the public hospital and private sector. Only 10% of bed capacity will be reserved for patients who are charged subsidised public healthcare prices, while the rest will be charged market prices (in excess of what is reimbursed by social health insurance). The private sector is responsible for financing, constructing, operating and managing the new medical center. The public hospital is responsible for sharing land, brand name of public hospital, patients, equipment, medical staff as well as managing and operating professional activities. Both the private and public sectors will be responsible for medical examinations and treatment. Identifying CVC opportunities in public hospital: Core services: The project will provide public health care services to the general population. Commercial potential and demand: The project is located in one of the most populous provinces in the country with high medical demand. There is a growing demand for faster and higher quality services from the middle-income population and commercial services from a large number of hospital staff. The hospital can mobilize revenues from private healthcare, office space for specialist clinics, advanced imagery facilities, parking and retail services provided to patients and hospital staffs of these various facilities. Beneficiary and stakeholder needs mapping: The mapping is shown in table below. Users Patients Regular health care services N/A (core revenue) Public health service fee covered by health insurance High-income Patients Improved health care services (similar to private hospital) Higher medical service fee Higher health service fee from high-income patients Stakeholders Hospital staff Access to facilities and amenities Retail (pharmacy, supplemental), food and beverages, convenience stores Rental fee from commercial space New hospital Access to equipment, staff, utilities Existing hospital can share staff, equipment, laboratory, imaging and other utility services. Medical equipment fee, lab service fee, profit sharing Assessing the policy, legal, institutional readiness in the country Policy and planning There is clear policy direction to mobilize private funding for hospital facility investment at all levels. High opportunity: Policy, legal and institutional framework are supportive and allow for CVC to be considered in the project. Next Step: Identify and analyse CVC in feasibility stage. Legal Framework There is existing legal framework to allow private participation in the provision of health services under various modalities. Institutional readiness Project Owner and players in the sector have extensive experience partnering with the private sector to deliver private health services under different commercial structures. Technical design: There are CVC opportunities for both the new and existing hospitals. For the new hospital, CVC opportunities are integrated in the project design to introduce modern facilities and commercial activities. The new hospital can be designed to allow for sharing infrastructure (lab, utilities, medical staff) with the existing hospital which will provide additional revenue for the existing hospital. Commercial feasibility: Based on a hypothetical assessment, the core revenue which is the user fee will come from medical service fee at mandated prices covered by public health insurance. As shown in the table below, the core revenue is 5% of total revenue required as the project is designed to primarily serve affluent groups and only allocate 10% of capacity to provide public health care services. As the new hospital will mainly cater to higher-income groups, it is aimed to be fully funded by commercial revenue. CVC will be in the form of commercial core services, commercial use of project space and infrastructure sharing, which will add 95% of total revenue required. The high share of revenue from commercial health care services provision is generally observed given higher revenue per patient in private hospital compared to public hospital. A. Core Revenue User Fee Medical service fee at mandated public health care prices (10% of beds) 5% B. CVC Commercial core services Higher medical service fee (in excess of mandated public health care prices) 90% Commercial use of physical space Rental fee from commercial space 5% Implementation: This project including CVC will be implemented through a joint venture scheme. A new JV will be established to invest in the new hospital with the private investor holding the majority share and the public hospital holding minority share. The public hospital’s contribution will be in the form of land value, branding and medical staff. The public hospital is legally allowed to set up a new company with a private company. Risks: The focus on high-income patients and sharing of resources (e.g., skilled doctors) with the private hospital may dilute the quality of core services, i.e. the public health objectives of the existing hospital. Footnote 1: The Worked Examples is hypothetical project business cases and include hypothetical financial assessments with key project information.Worked Example 3: Public Hospital
Groups
Description
Need
CVC Opportunities
Revenue Streams
Areas
Assessment
Level
Revenue Category
Revenue Item
Expense Items
Net revenue as % of total revenue1
The Guidelines on Innovative Revenues for Infrastructure (IRI) is intended to be a living document and will be reviewed at regular intervals. They have not been prepared with any specific transaction in mind and are meant to serve only as general guidance. It is therefore critical that the Guidelines be reviewed and adapted for specific transactions.
To find more, visit the Innovative Revenues for Infrastructure section and the Content Outline, or Download the Full Report. For feedback on the content of this section of the website or suggestions for links or materials that could be included, please contact the PPPLRC at ppp@worldbank.org.
![]()
Updated: February 23, 2024